CASE STUDY 3
Author

Professor Dr.med. Jens Tischendorf Chief Physician at the Department of Internal Medicine and Gastroenterology Rhein-Maas Hospital
Würselen, Germany
Patient's Medical History
The patient was admitted with colicky upper abdominal pain and slightly elevated cholestasis test results. As the patient underwent a Billroth II gastric resection and Roux-en-Y anastomosis many years ago, magnetic resonance cholangiopancreatography (MRCP) was initially performed which revealed a large concretion in the ductus hepatocholedochus (DHC).
Endoscopic Intervention with Dilatation
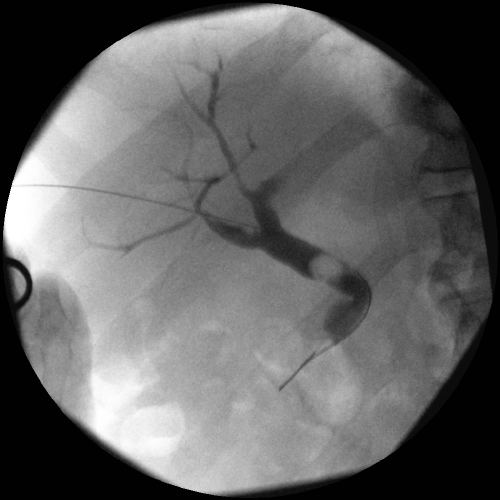
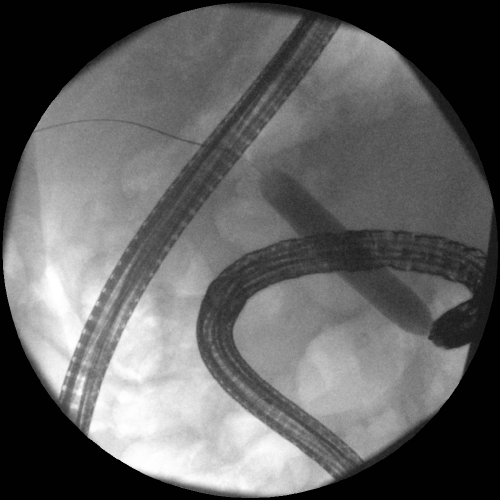
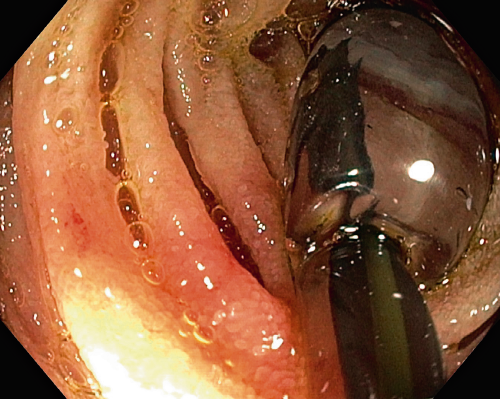
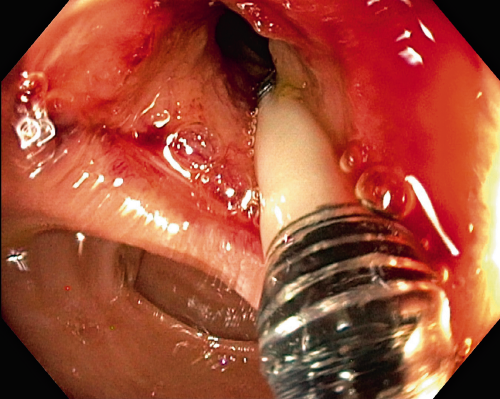
Since, due to the anatomical anomaly, it was not possible to approach the papilla of Vater with the endoscope sufficiently well to explore the DHC, we performed percutaneous transhepatic cholangiography drainage (PTCD) which, as expected, revealed a large stone in the DHC (Fig. 1). After advancing the percutaneously introduced wire into the small bowel, it was possible to grip the wire using a pediatric colonoscope (Olympus PCF-190L) in a rendezvous procedure. This now provided safe access to the bile duct and the next step was the gradual balloon dilatation of the papilla with the Olympus EZDilate BD-410X-1355 to a maximum diameter
of 13 mm (5.5 atm) (Fig. 2 and 3). A sufficiently wide ostium papilla with a direct view into the DHC was then found (Fig. 4) so that the stone could now be easily extracted by transpapillary removal using a small basket. The final cholangiogram showed the DHC to be free of stones (Fig. 5).

Procedure and Summary
The EZDilate balloon dilator allows controlled, gradual dilatation of the papilla of Vater, which facilitates endoscopic intervention in difficult bile duct situations, as in our case with an altered anatomy and a large DHC concretion.
- Content Type