DESCRIPTION OF TECHNIQUE
Placement in the Operating Room
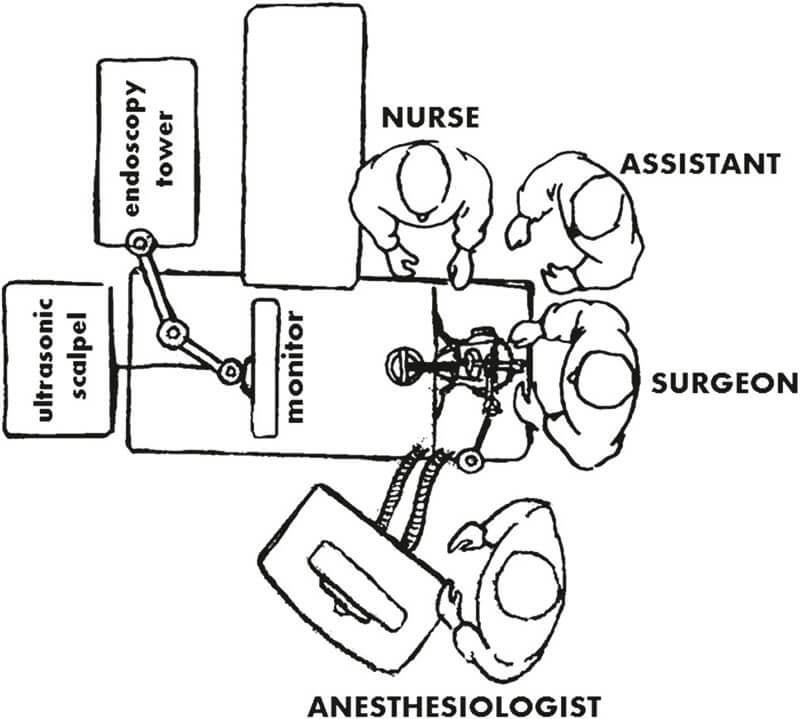
The patient is placed in the supine position. Cervical extension will be avoided so the surgical field in the pharynx may be as broad as possible. The respirator and anesthesia will be to the left of the patient. Behind the general anesthesia, the arm holder will be placed to the left of the patient with the end not impeding the passing of material between the nurse, situated to the right of the table, and the surgeon, situated at the head. The assistant will place himself to the left or right of the surgeon, as needed. The THUNDERBEAT system (ultrasound / advanced bipolar) should be placed at the foot of the operating table and the endoscopy tower to its right to allow easy access. The tower monitor has a jointed arm that allows for its placement on the axis of the surgical table and closer to the surgeon. The sterile table will be positioned toward the foot of the surgical table so that the nurse can also be facing the screen and can follow the procedure.
Placement of the FK-WO Retractor

The FK-WO laryngo-pharyngoscope creates pharyngolaryngeal space by means of the anterior retraction of the base of the tongue or the supraglottis. The different types of retractor blade allow for a more adequate exposure of each lesion according to its location.
Endoscope Placement and Use
The ENDOEYE FLEX 5 mm videoscope, providing 100° angulation in four directions, is introduced through the retractor to obtain an adequate image of the lesion. The position of the videoscope is stabilized with the arm holder fixed to the left side of the table. It is possible to refine the image through movement of the distal end of the endoscope.


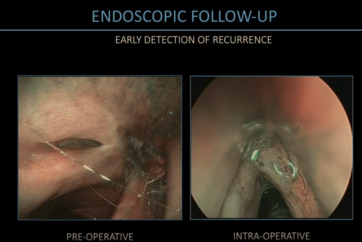
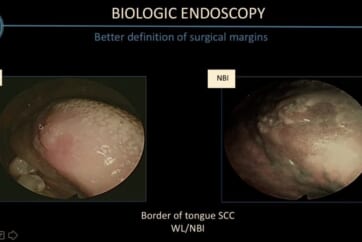
Support Through NBI Endoscopy
Endoscopic visualization allows the mucous membranes and the lesion to be approached more closely and the macroscopic characteristics of the area to be looked at closely before deciding the extent of the resection. The NBI light is a tool incorporated into the videoendoscopy that allows the vascular structure characteristics of the mucous membranes and the lesions to be evaluated. The vascular structure will help both to differentiate the malignant or benign nature of the lesions and to define them. TOUSS as an endoscopic technique can use NBI technology simultaneously during the procedure, so the surgeon can better delineate the extension of the resection.
Using THUNDERBEAT Type S for Tissue Resection
THUNDERBEAT Type S will be used to resect the tissue, assisted by the laparoscopy instruments. The basic forceps are 35 cm, although for even closer lesions the 20 cm forceps may be more convenient. The rigid suction pump will be handled by the assistant to keep the field clean and flush the aerosol. Nevertheless, it can also be used by the surgeon as a support instrument.


- Content Type