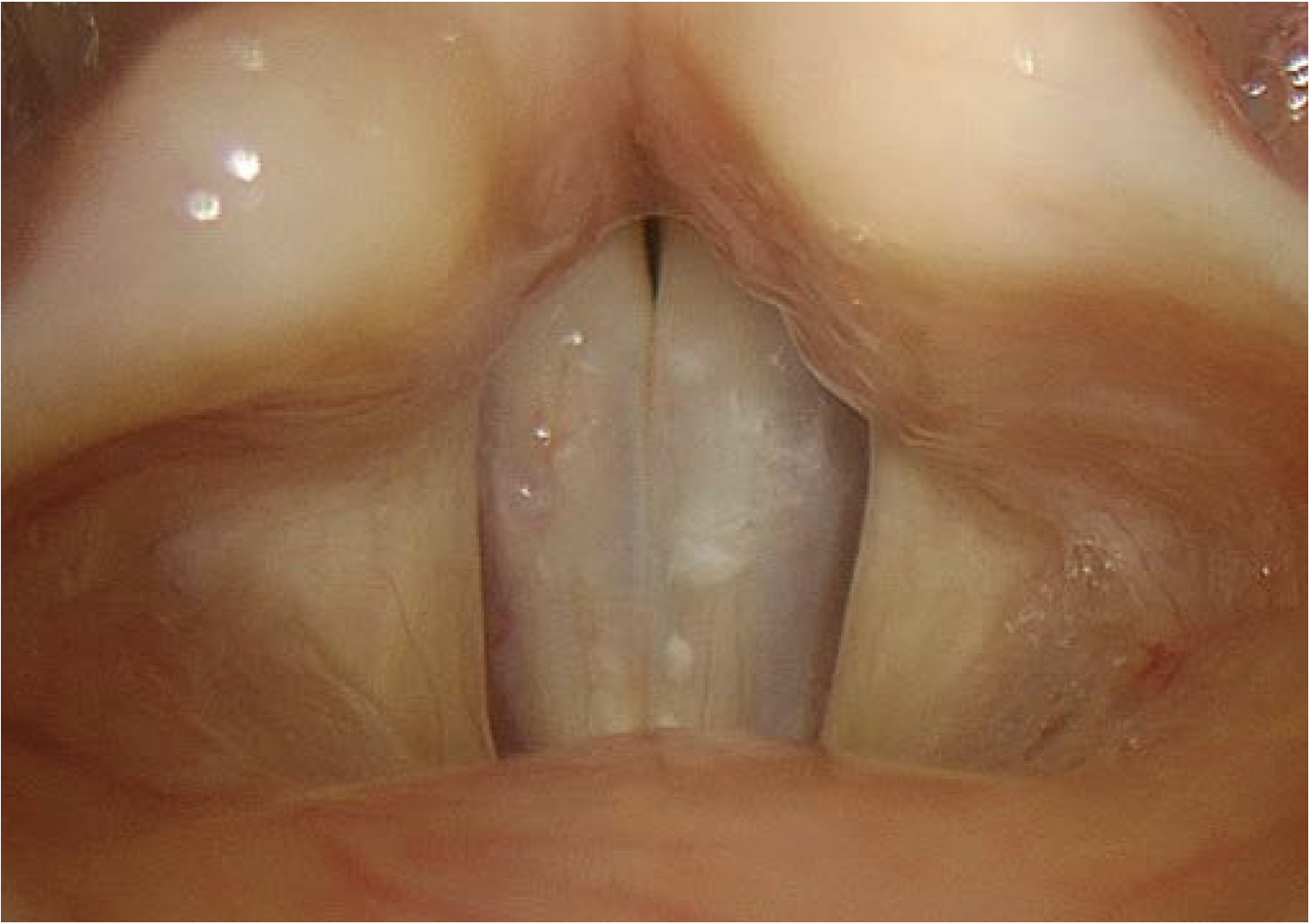
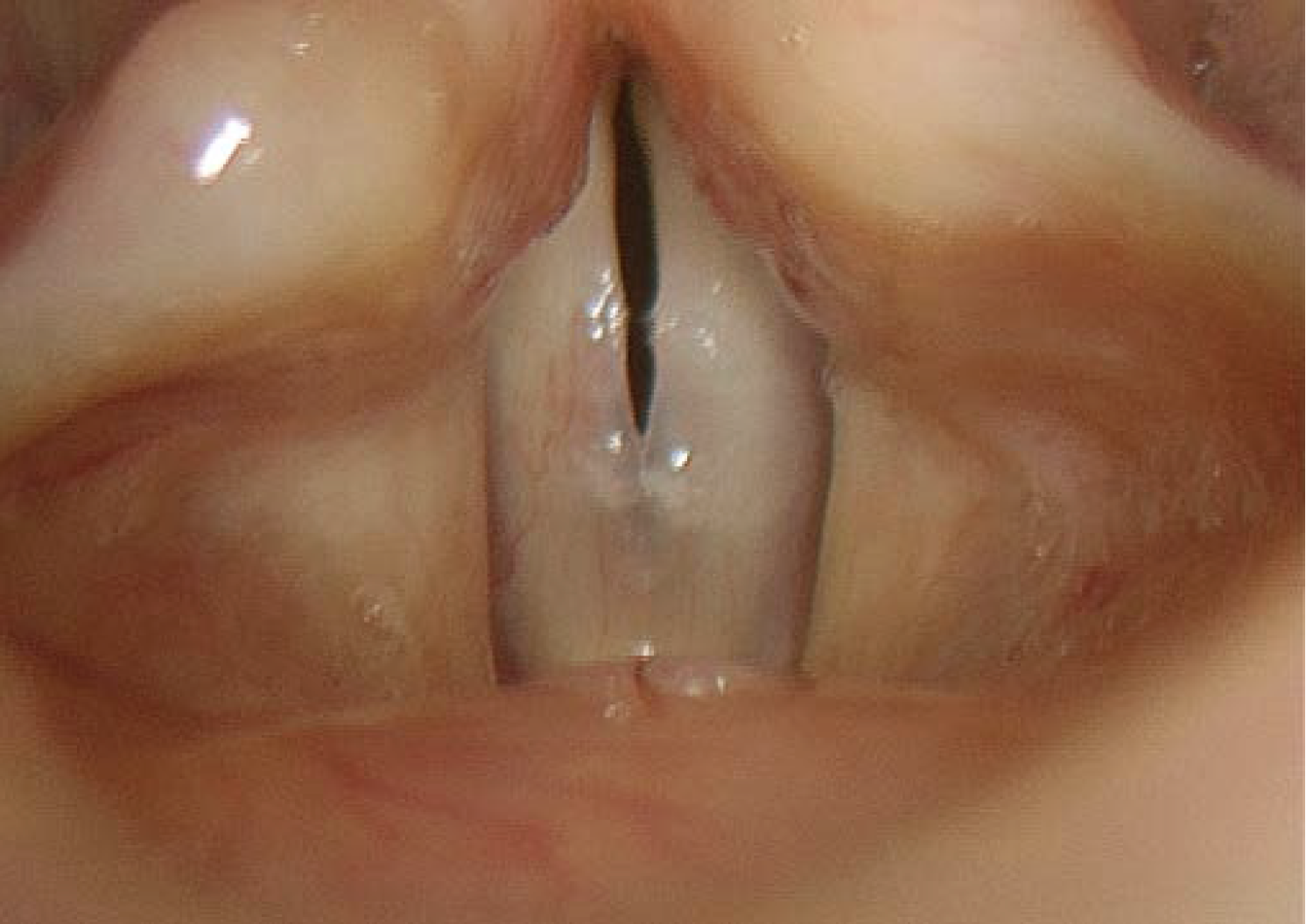
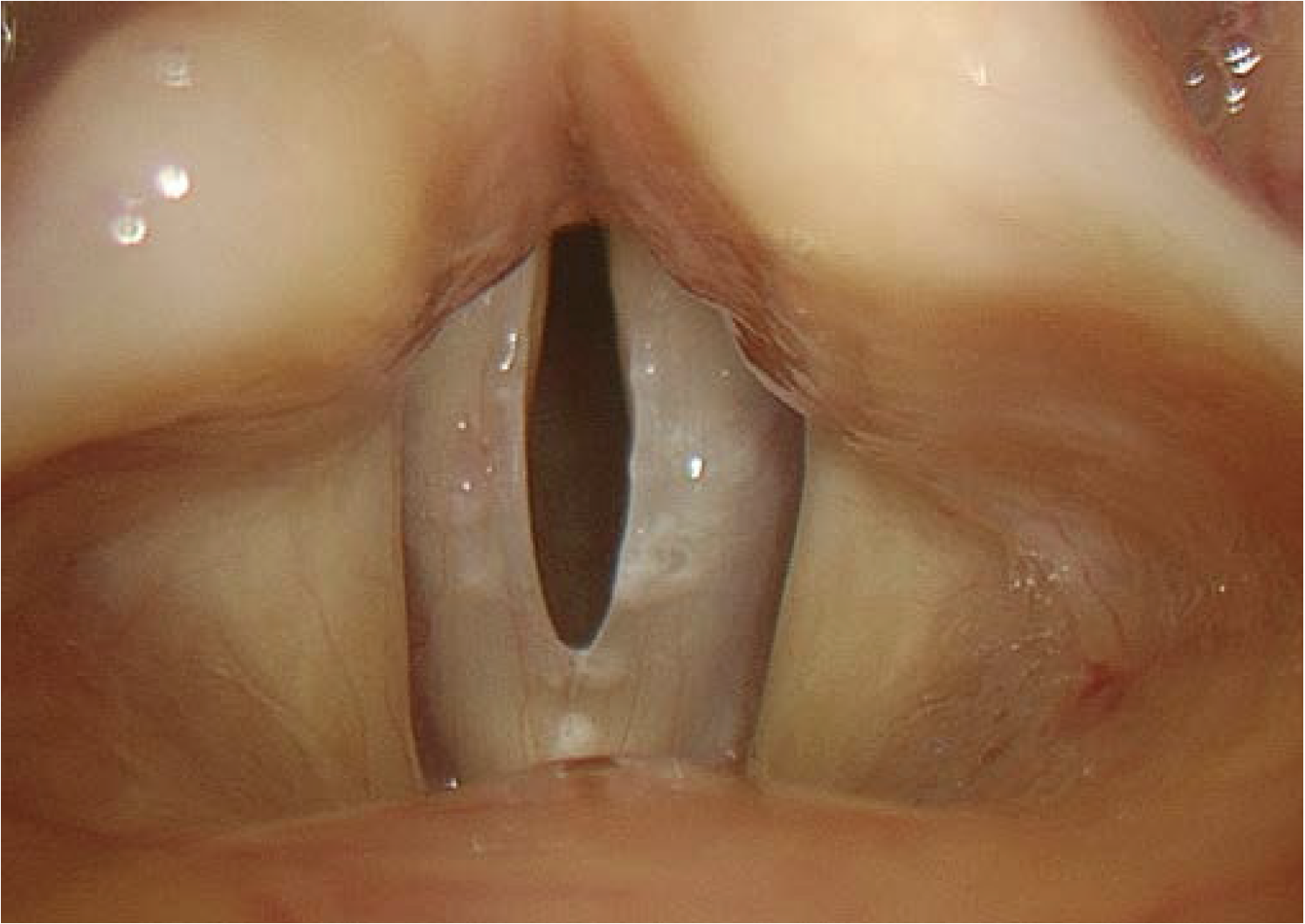
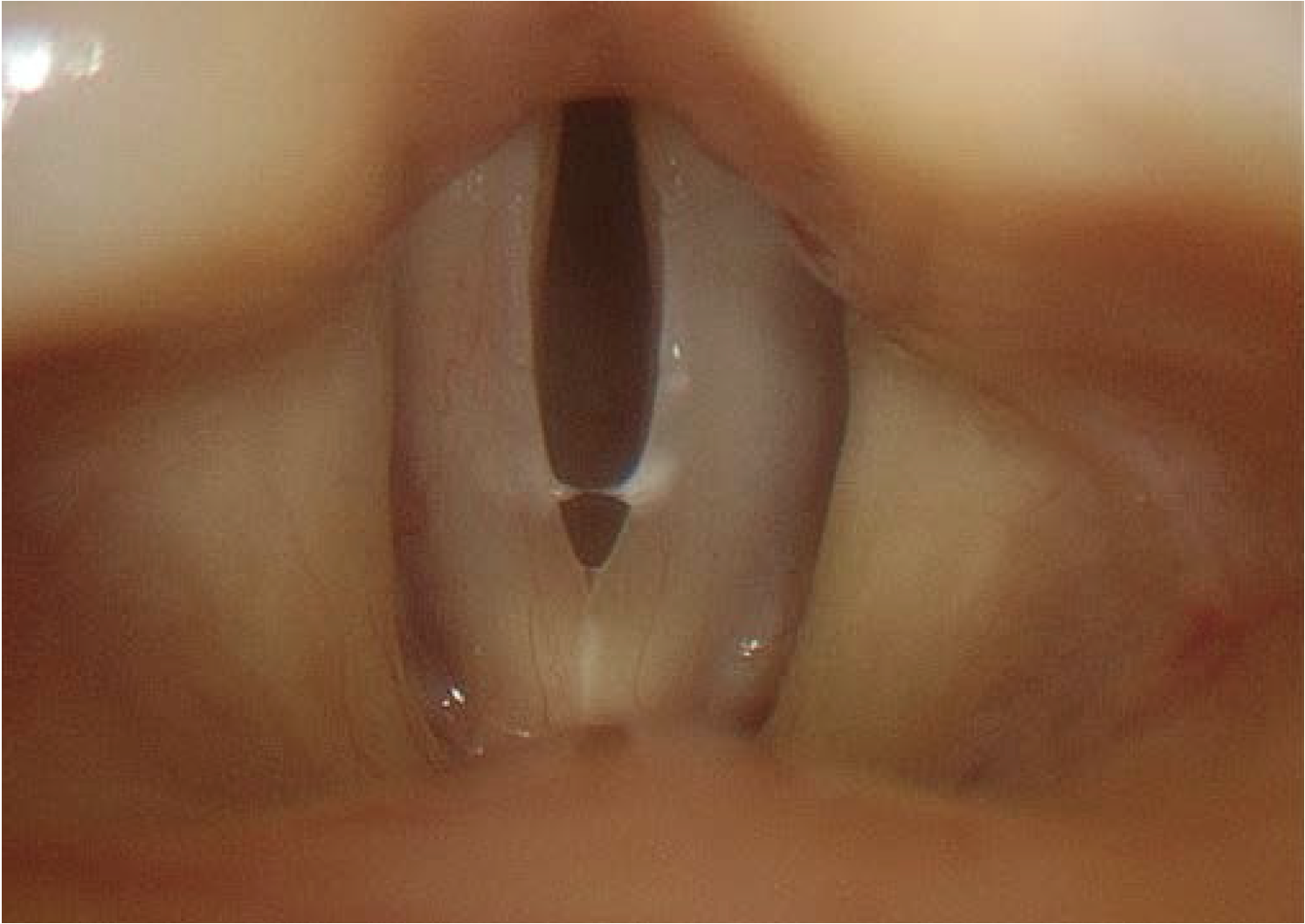
STROBOSCOPY
We would need a whole book to describe the technique of stroboscopy and all of its advantages. Unfortunately, it is only possible to cover some aspects in this section. Stroboscopy is an essential tool for the evaluation of mucosal waves and the pliability of the tissue of the vocal fold cover. Minor alterations in the normal waveform may provide the only sign that there is a mechanical problem. It may therefore help to distinguish organic voice disorders from functional disorders.
Some technical details should be considered:
Check for different pitches and various loudness levels.
Use moving mode and fixed mode.
Most patients stop phonation after one or two seconds – that is too short for thorough evaluation of the vibratory functions.
For example say to the patient: “Please give me an “eee” for 10 seconds.”
Stroboscopy in patients with aphonia or with a very hoarse voice does not make sense.
Voice recording and documentation of fundamental frequency and sound pressure level are essential – you want to know which sound was produced when assessing vocal fold vibration.
Useful Technical Terms in Stroboscopy
- Pulsed vs. CW (continuous wave) light
- Halogen vs. xenon light
- Slow vs. fast motion
- Fixed vs. moving mode








Important Criteria in Stroboscopy:
→ Symmetry of Vocal Fold Movement
– Phase symmetry / asymmetry, phase difference
– Abnormal modes of vibration
– Alternating vibration
→ Periodicity of Vocal Fold Movement
→ Regularity of Vibration
→ Amplitude of Vocal Fold Movement
– Symmetrical
– Normal / diminished / extended
– Absent
→ Mucosal Wave
– Symmetrical / asymmetrical
– Normal / diminished / extended
– Absent
→ Glottic Closure (vocal fold closure)
– Complete / incomplete
→ Open Quotient
→ Glottal Gap
– Posterior / anterior / elliptical / hourglass
→ Nonvibratory Mucosa / Stiffness
Alternatives:
Alternatively to stroboscopy, imaging of the vibratory behavior of the vocal folds is possible with video kymography (VKG) and high-speed imaging.


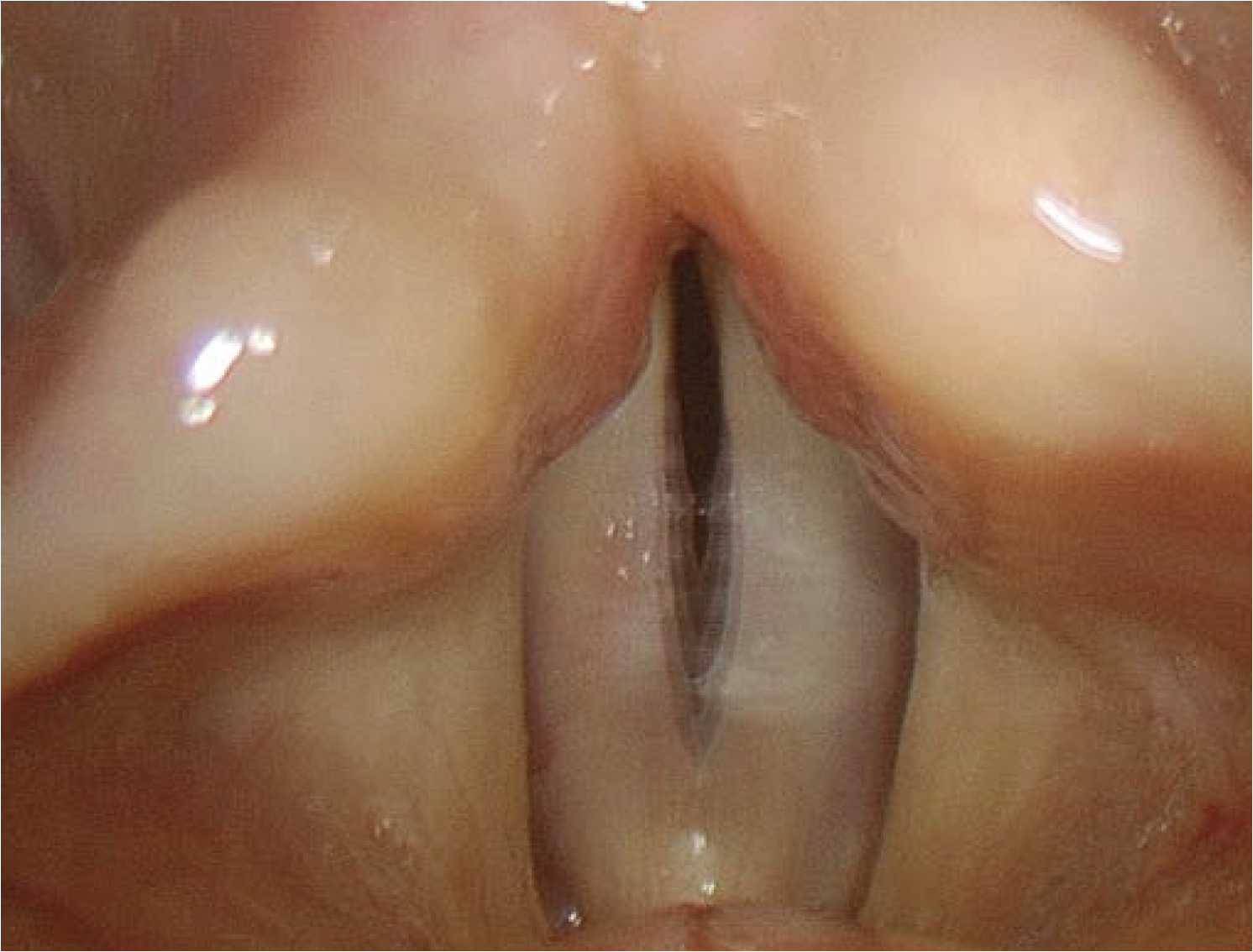
Images obtained using a stroboscopic flashlight source have a slightly more blue quality than those obtained using a continuous wave light source. This discrepancy can easily be corrected by digital image processing. In addition, the images may be somewhat darker than those obtained using a continuous light source. Image quality is generally improved by getting the tip of the endoscope as close to the vocal folds as possible.
- Keyword
- Content Type